Pipe handling frame incident during diving operation
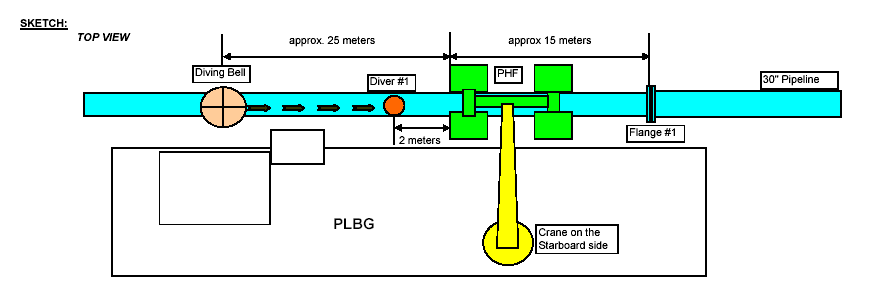
A member has reported an incident while a pipe handling frame (PHF) was being lowered to a depth of 100 metres from a barge using its starboard crane when a shift change was in process onboard. At the same time, a diving bell was at the depth of 155 metres, 25 metres away from the descending PHF area.
A diver left the bell and went to the seabed (depth 169 metres) and proceeded to the location of a flange to perform his task. This put him approximately 40 metres away in the direction of the descending PHF.
As the diver was moving towards the flange, he noticed cloud of ‘muck’ 2 metres away from him.
He immediately stopped and informed his supervisor. In the process, he made physical contact with the PHF, which had settled half on the pipeline and the seabed.
No injuries was sustained to the diver or damage done to the 30″ pipeline.

The member has noted the following related points:
- at the time of the incident, a shift change was in process;
- the PHF dimension was 5.60m 5.20m 2.50m, its weight in air 18 tons and its weight in water 16.5 tons;
- the PHF was being lowered at a speed which was disabling the transponder needed to update the survey system;
- the transponder used to monitor the lowering and rising of loads and crane wires malfunctioned (sending intermittent signals).
The following investigation reached the following conclusions:
- The diving supervisor taking over shift and managing the subsequent lock-out of the diver could not reasonably be expected to know the situation of the PHF, other than that it was as planned, without another person informing him of any subsequent change, i.e. the deck foreman or the survey operator;
- The action to over-board the PHF and ‘park it’ at 100m until the supervisor could take control was a sensible and prudent administration strategy;
- The fact that the PHF was not parked at 100m should have been noted and passed to the supervisor by the crane operator and the survey team.
- The diving supervisor should have verified the position of the PHF prior to locking out the diver. Instead, he relied on the crane operator and the survey systems to manage the position of the PHF.
- The diving supervisor was negligent in locking out the diver and progressing the diver to the work location with the PHF suspended at the proposed 100m level.
Safety Event
Published: 1 October 2004
Download: ![]() IMCA SF 09/04
IMCA SF 09/04
IMCA Safety Flashes
Submit a Report
IMCA Safety Flashes summarise key safety matters and incidents, allowing lessons to be more easily learnt for the benefit of all. The effectiveness of the IMCA Safety Flash system depends on Members sharing information and so avoiding repeat incidents. Please consider adding safetyreports@imca-int.com to your internal distribution list for safety alerts or manually submitting information on incidents you consider may be relevant. All information is anonymised or sanitised, as appropriate.
IMCA’s store terms and conditions (https://www.imca-int.com/legal-notices/terms/) apply to all downloads from IMCA’s website, including this document.
IMCA makes every effort to ensure the accuracy and reliability of the data contained in the documents it publishes, but IMCA shall not be liable for any guidance and/or recommendation and/or statement herein contained. The information contained in this document does not fulfil or replace any individual’s or Member's legal, regulatory or other duties or obligations in respect of their operations. Individuals and Members remain solely responsible for the safe, lawful and proper conduct of their operations.