Near miss: diver’s umbilical trapped
What happened?
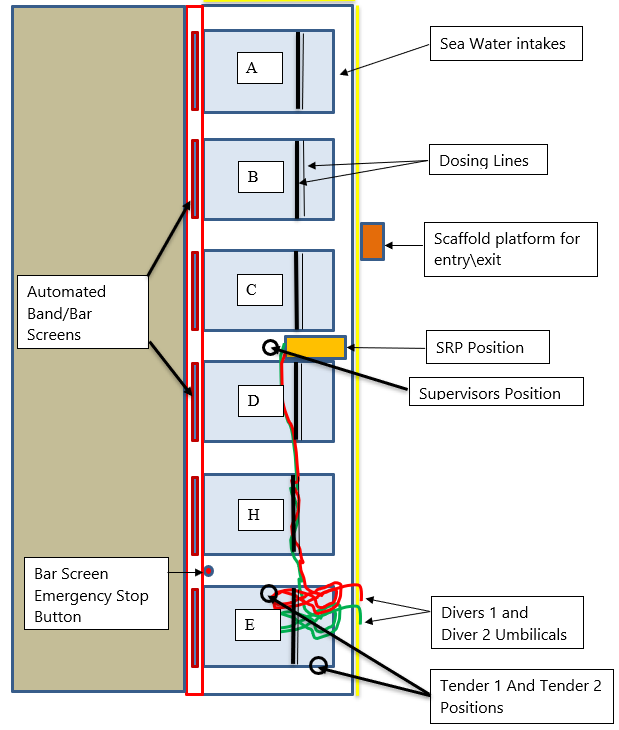
During near-shore diving operations, a divers’ umbilical became trapped against a seawater intake. The dive team (2 x divers, 2 x tenders and dive supervisor) had completed a task and were busy recovering all the tools and rigging to recover to surface. Both tenders were receiving the tools from the water, and both diver’s umbilicals were briefly secured to a railing. Diver 1 was looking for any tools left behind on the seabed when his excess (untendered) umbilical drifted into one of the seawater intake channels and lay against the screen. The automated bar started and Diver 1’s umbilical became trapped. The rotating bar emergency stop button which was less than 10m away from dive control was immediately used by the dive supervisor. Diver 1 transferred onto his bailout and upon confirmation that the band screen was stopped, Diver 2 approached to assess the situation. The bar screen was manually turned in reverse, in order to free Diver 1’s umbilical.
Onsite client personnel manually reversed the band screen direction before both divers returned to surface, and diving operations were suspended. There were no injuries sustained to either diver and upon inspection of the umbilical, there was a small perforation in the main airline approximately 11m from the helmet. The communications cable also sustained cut damage.
What went wrong? What were the causes?
- Contributing factors:
- diver umbilicals were tied off on the railing and were not being actively tendered; tenders were onsite but were engaged in other activities at the time (tender 1 was removing lifting gear and equipment from the crane hook, tender 2 was recovering tools using the messenger line)
- seawater intakes were not isolated;
- Immediate causes:
- there was no isolation of bar screens on the seawater intakes before diving began
- umbilicals were not being actively tendered;
- Diver 1 failed to monitor his umbilical slack whilst he was engaged in recovering tools;
- Root causes:
- inadequate engineered controls: failure to implement suitable equipment isolation
- inadequate oversight or supervision.
What actions were taken? What lessons were learned?
- Thorough review and revision of risk assessment for this work;
- Revision of dive log requirements to include appropriate work planning and appropriate permit to work (PTW) requirements;
- Debrief and formal review by dive team, of method statement, dive plan and risk assessment, with particular reference to:
- umbilical management
- isolation of sea water intakes/band screens
- are there enough people involved?
- ‘last minute’ risk assessment
- guarding against complacency and the hazards of ‘routine’ activities.
Members may wish to refer to:
Safety Event
Published: 23 August 2019
Download: ![]() IMCA SF 20/19
IMCA SF 20/19
IMCA Safety Flashes
Submit a Report
IMCA Safety Flashes summarise key safety matters and incidents, allowing lessons to be more easily learnt for the benefit of all. The effectiveness of the IMCA Safety Flash system depends on Members sharing information and so avoiding repeat incidents. Please consider adding safetyreports@imca-int.com to your internal distribution list for safety alerts or manually submitting information on incidents you consider may be relevant. All information is anonymised or sanitised, as appropriate.
IMCA’s store terms and conditions (https://www.imca-int.com/legal-notices/terms/) apply to all downloads from IMCA’s website, including this document.
IMCA makes every effort to ensure the accuracy and reliability of the data contained in the documents it publishes, but IMCA shall not be liable for any guidance and/or recommendation and/or statement herein contained. The information contained in this document does not fulfil or replace any individual’s or Member's legal, regulatory or other duties or obligations in respect of their operations. Individuals and Members remain solely responsible for the safe, lawful and proper conduct of their operations.