Uncontrolled movement of a riser
What happened?
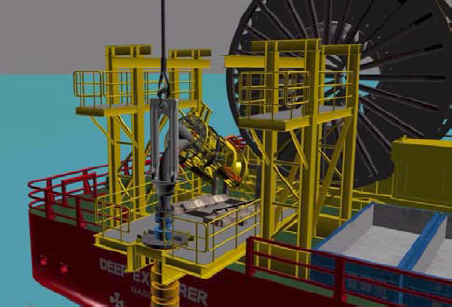
A riser moved unexpectedly away from the vessel. The incident occurred during the deployment of a production riser from a hang-off frame located starboard aft. All rigging had been connected and the crane had taken the load and slewed inboard to allow the removal of the hang-off plates and beam. A 3-tonne lever hoist was also attached to assist in this activity. The rigging team were about to remove the chain hoist (before slewing the crane outboard) when there was an unexpected sudden movement of the riser to starboard. The chain hoist parted and the riser moved clear of the hang-off platform to approximately 8m off the vessels side.

What went wrong? What were the causes?
The proposed arrangement had been risk assessed and it was noted that the riser was leading away from the vessel (this was in line with the written procedure). A decision was made to install a bellyband (soft sling) around the riser which would be connected to a lever hoist. This would be used to steady the riser to assist the riggers in the removal of the hang-off collars and beam. This rigging was arranged and secured to the riser end fittings and the process of deployment continued. The bellyband was in addition to the existing procedural requirements, but there had been no management of change (MoC) process followed for this addition.
The crane was slewed inboard to allow the removal of the beam (as per procedure). Once the hang-off collars and beam had been removed, the crane operator requested a movement outboard as he was concerned with the 3° side lead on the crane wire. The confirmation was to move the crane outboard ‘just a touch’. Two personnel remained in position to remove the additional rigging. The CCTV footage showed the crane slew to the left and come to a stop. Almost immediately, the bellyband lever hoist failed. The riser suddenly moved left, bending a section of handrail on the hang off platform as it moved.
Our members’ investigation concluded that the causes of the incident were a lack of risk perception and the failure to follow procedures (engineering and MoC). Key points include:
- The introduction of the bellyband rigging was not identified as a change and therefore was not managed via the MoC process;
- The effects of moving the crane jib on the riser were not considered;
- As the risk was not identified and managed via the MoC process, once the movement of the riser began, the 3-Tonne lever hoist was not sufficient to prevent the incident from occurring;
- There was ineffective communication between the rigging supervisor and the crane operator;
- It was important to ensure supervisor involvement in shift briefings and toolbox talks (TBT) and communicating relevant information which allowed personnel to understand the task (step by step) and hazards associated with each step.
What actions were taken? What lessons were learnt?
- A clear task outline should be provided so that all personnel involved understand all the steps involved;
- Instructions should be precise, accurate and free of ambiguity;
- Any change, no matter how small, should be subject to the MoC process.
Members may wish to refer to the following incidents:
- High potential stored energy incident: inner buoyancy module clamp failure during removal [involving work on a riser where changes to the work process were not subject to a Management of Change process.]
- Lost time injury (LTI): Rigger struck by rigging under tension [in which the investigation identified the need to identify and mitigate all risks associated with a Management of Change (MoC) process.]
Safety Event
Published: 4 June 2018
Download: ![]() IMCA SF 11/18
IMCA SF 11/18
IMCA Safety Flashes
Submit a Report
IMCA Safety Flashes summarise key safety matters and incidents, allowing lessons to be more easily learnt for the benefit of all. The effectiveness of the IMCA Safety Flash system depends on Members sharing information and so avoiding repeat incidents. Please consider adding safetyreports@imca-int.com to your internal distribution list for safety alerts or manually submitting information on incidents you consider may be relevant. All information is anonymised or sanitised, as appropriate.
IMCA’s store terms and conditions (https://www.imca-int.com/legal-notices/terms/) apply to all downloads from IMCA’s website, including this document.
IMCA makes every effort to ensure the accuracy and reliability of the data contained in the documents it publishes, but IMCA shall not be liable for any guidance and/or recommendation and/or statement herein contained. The information contained in this document does not fulfil or replace any individual’s or Member's legal, regulatory or other duties or obligations in respect of their operations. Individuals and Members remain solely responsible for the safe, lawful and proper conduct of their operations.